


Other Parts Discussed in Thread: ADS1292R,
Tool/software:
I see on the layout examples and the development kit that there are many passives on the input lines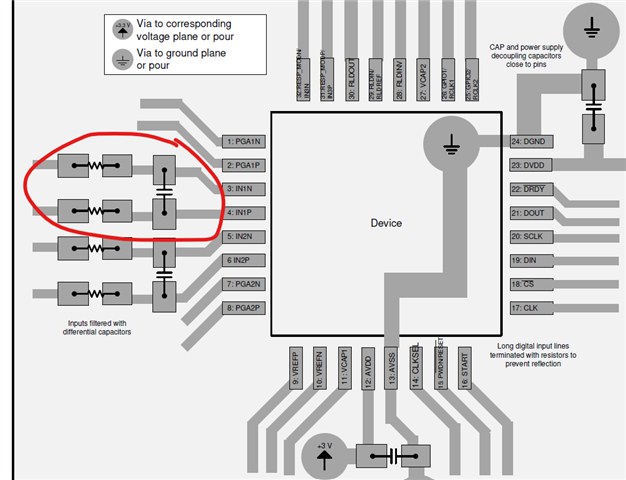
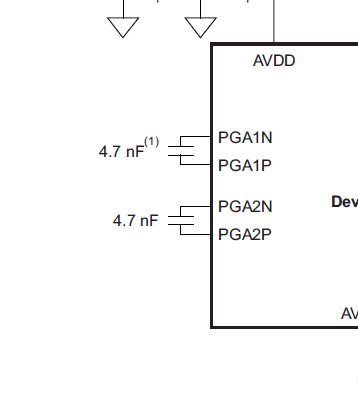 It looks to me like just a 4.7 nf is required and its suggesting some patient protecting resistors, is that correct?
It looks to me like just a 4.7 nf is required and its suggesting some patient protecting resistors, is that correct?
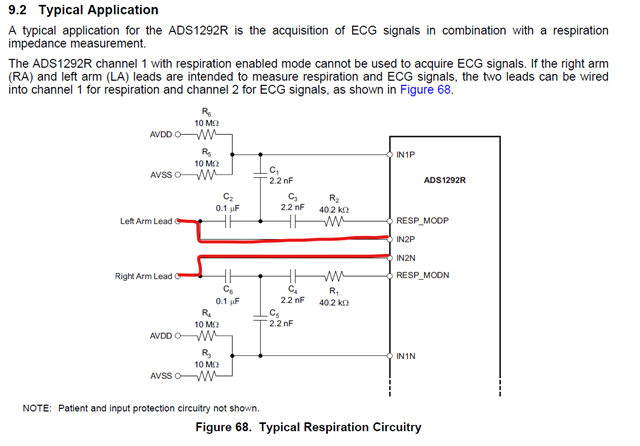
When i see the typical application it has an example with no passives if not using the respiratory functions. Is this example only relating to respiration?
Now when i look at the development kit im a bit taken back. 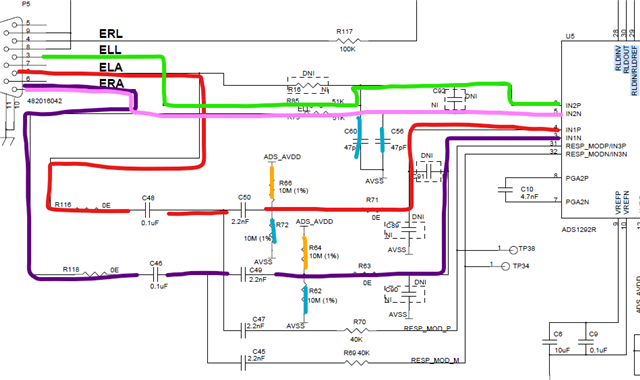
Out of these options, assuming i just want to use 2 electrode, one lead eeg. On my design i am just using IN1P and IN1N including the 4.7nf cap.
On the development kit i have been using ERA and ELA but this doesnt seem to match with what i intend to do.
It looks like I should be using ELL and ERA but on the development software my options are ● ECG Lead I
● ECG Lead II
● ECG Lead III
● ECG Lead aVR
● ECG Lead aVL
● ECG Lead aVF
I'm a bit confused reading through the documentation how these map to IN1P and IN1N.
Any help is appreciated.

