Part Number: ADS1298
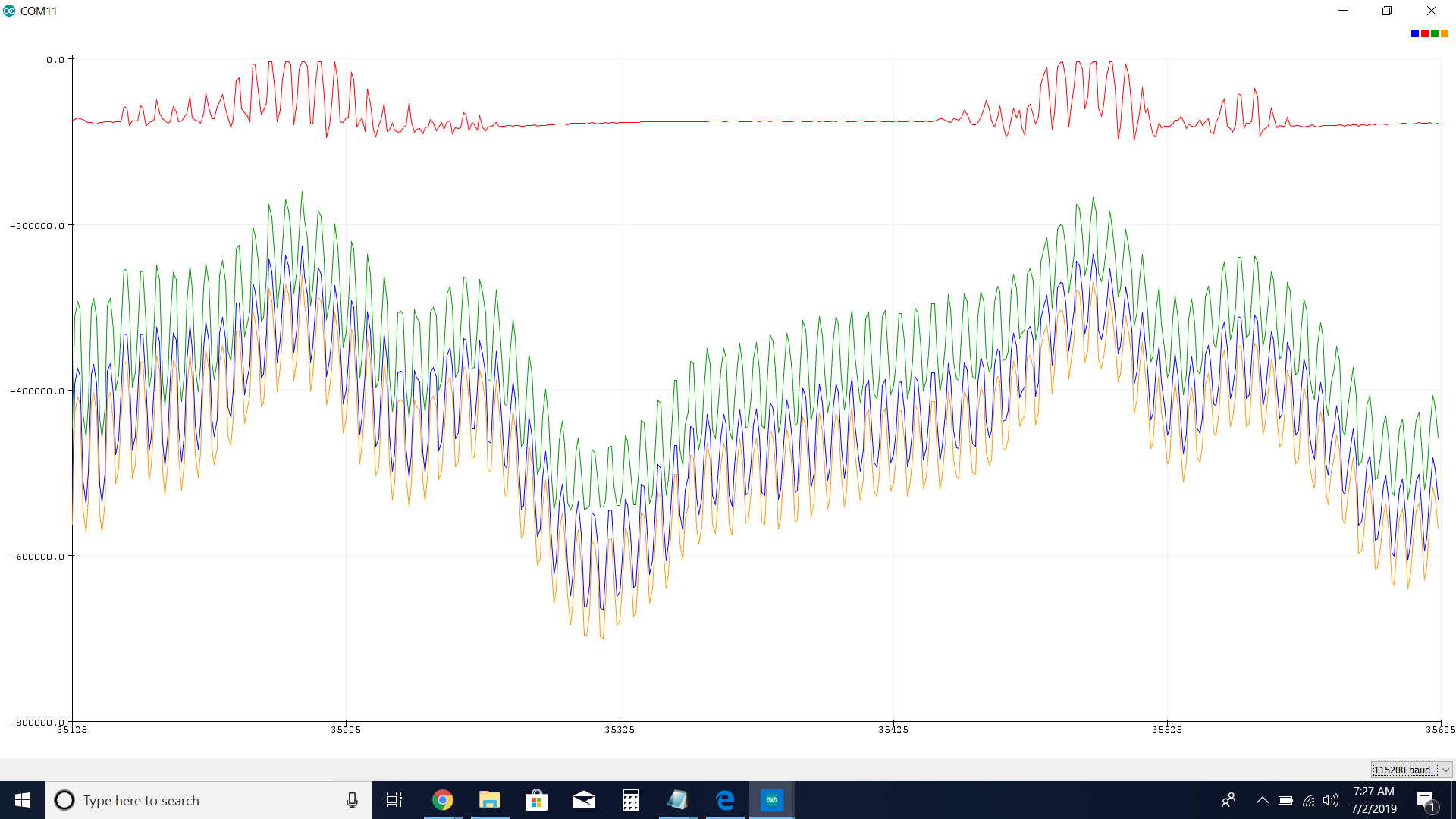
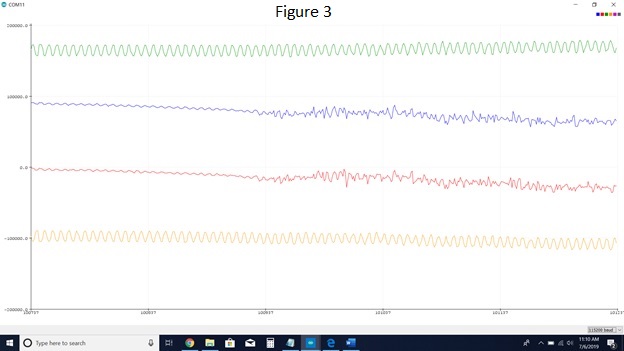
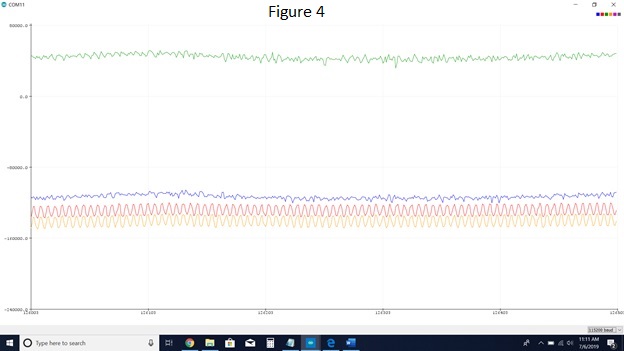
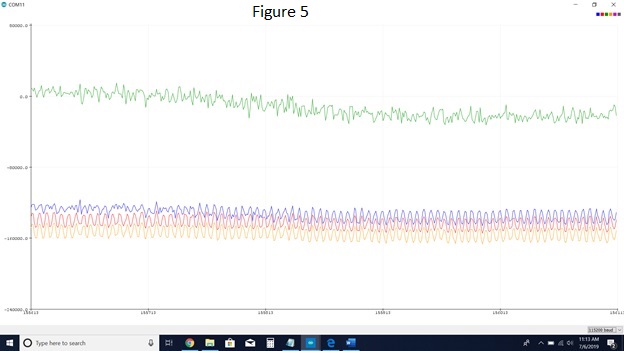
I am having problems with the RLD drive system. I am able to read signals, both computer generated and human generated. The issue I am having is that I have a lot of noise (possibly 60Hz noise) when I'm reading, and patient movement also generates a significant amount of noise. I read through the documentation for RLD drive, but I'm still missing some of the "how-to". I would like to use the RLD drive to get rid of the extra noise in my system.
Questions:
- To use RLD drive, should I be concerned with the CONFIG3 register or RLD_SENSP and RLD_SENSN registers?
- What settings should I put each channel in (in the CHnSET)?
- What channels should I have electrodes in?
Clarifications/Where I'm at:
- I will be using all the electrodes on the patient's forearm.
- I am using an ADS1298.
- I can easily read and write to registers.
- I am using an Arduino Due.
- I would like to use as many channels as possible.