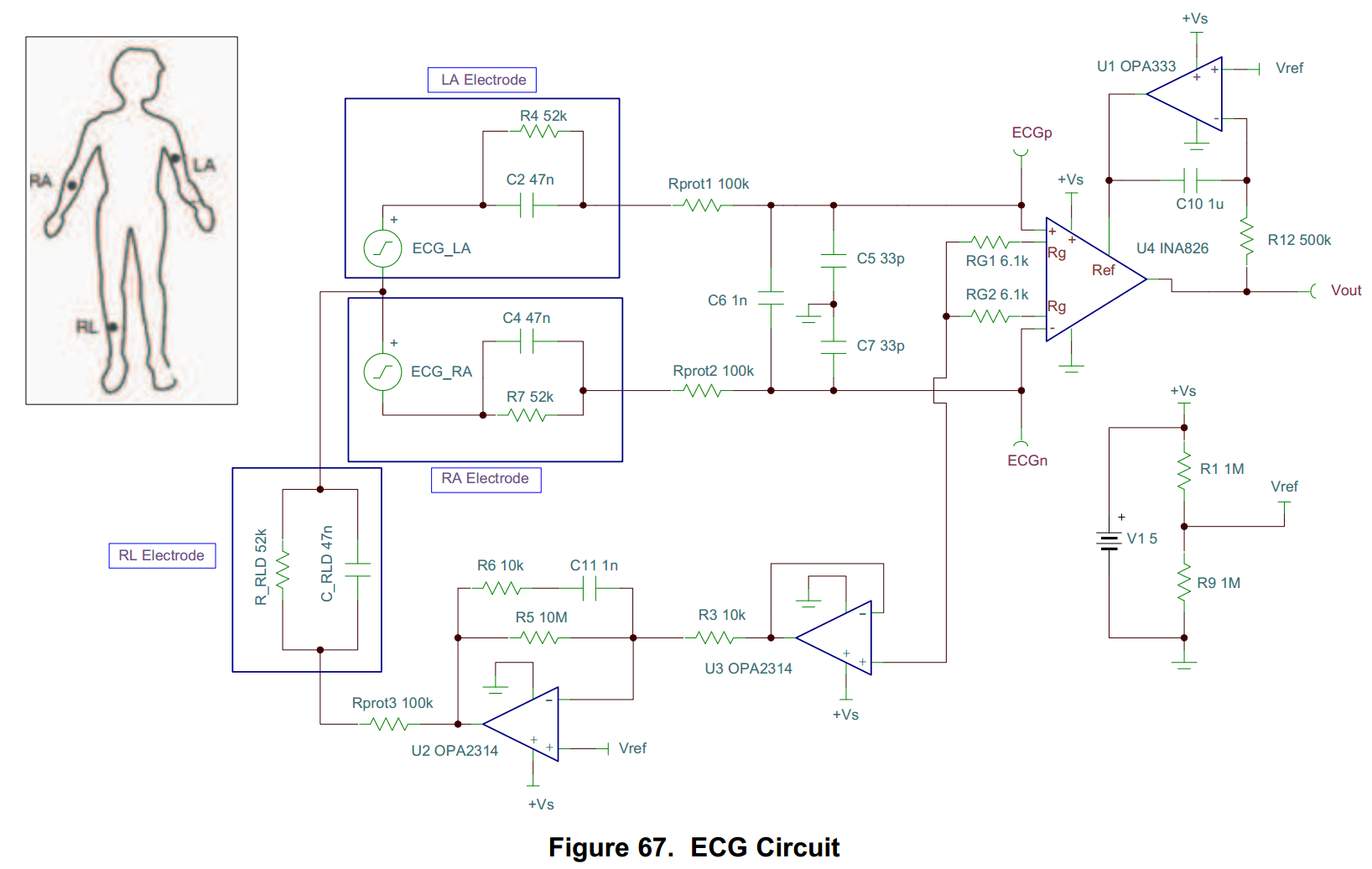
Looking at Fig 67 on p27 of the INA826 datasheet, there is a single-supply one-lead ECG circuit that uses OPA333 as an integrator to remove the DC component of the output signal, by inverting it and feeding it back to the reference input of INA826. I have three questions:
A.1) What is the reason for using OPA333 (which is a relatively expensive op-amp), rather than simply a ground reference (or low-impedance rail-splitter if single-supply) and a passive high-pass filter (or even an active high-pass filter with a much cheaper op-amp, such as OPA314). Does it somehow improve the input common-mode range, or cause an effective increase in the output voltage range?
A.2) What is the high-pass frequency for the circuit in Fig 67, and how do I calculate it? Is the slope of the cut-off filter the same as a one-pole passive high-pass filter? For diagnostic ECG it should be 0.05Hz; what combination of resistor and cap would be best for that?
A.3) What effect would there be on performance if I substituted a much cheaper op-amp, such as OPA314 in place of OPA333?
Second part:
B.1) If I wanted to use input buffer op amps before the INA826 (e.g. OPA314 simply as a unity gain buffer) would this reduce the performance at all? Could it improve it, by providing the INA826 all the bias current it could possibly require?
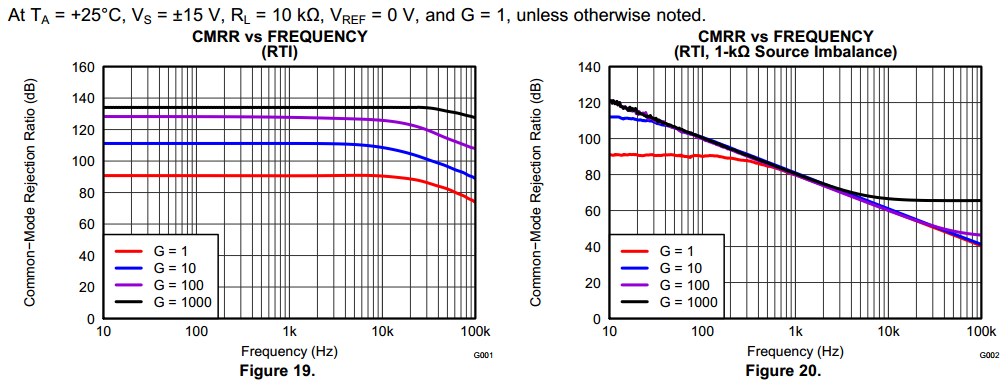
B.2) In a unity-gain buffer, does the CMRR of the op-amp matter at all? I have read in a published book that it is irrelevant in unity-gain, whilst an electronics engineer has told me it is still important.
Thanks!